Pituitary Adenomas: Prolactinomas and Hormone Imbalances Explained
 Mar, 5 2026
Mar, 5 2026
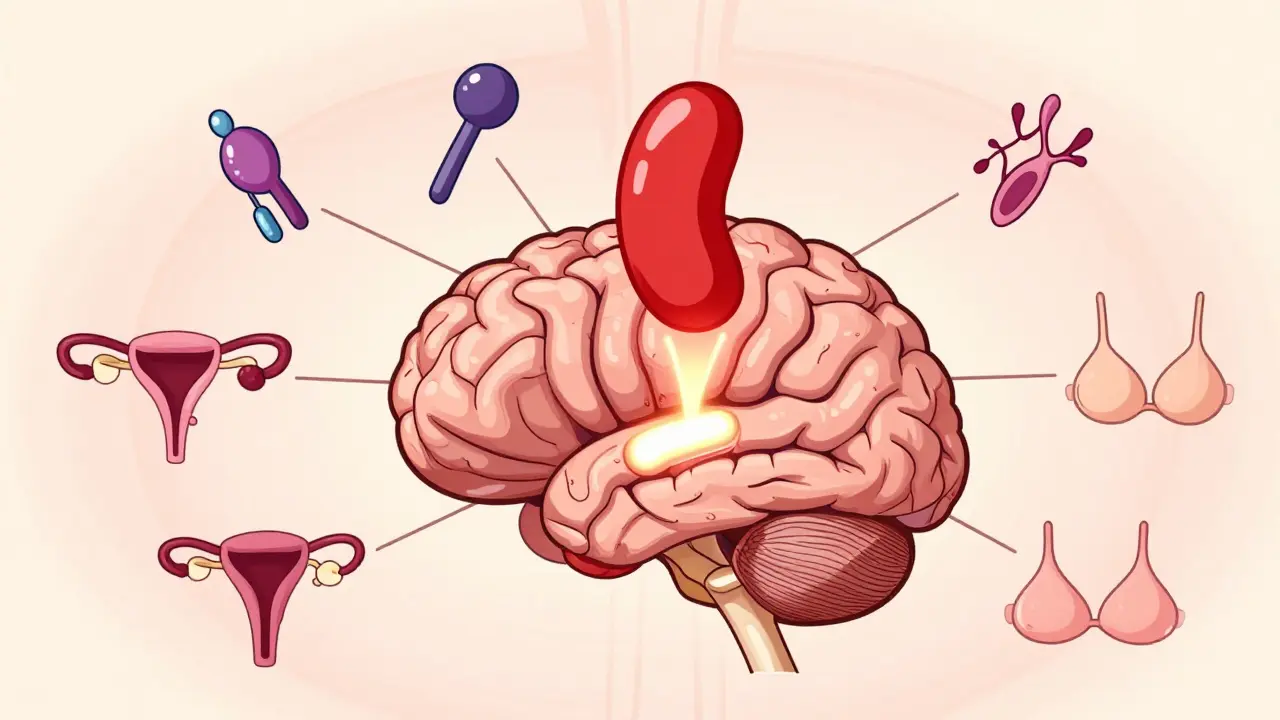
When your body’s hormone system goes off track, it’s rarely because of one simple thing. For many people, the culprit is hidden deep inside the brain - a small, pea-sized gland called the pituitary gland. This gland controls everything from your menstrual cycle to your stress response, and when a benign tumor called a pituitary adenoma forms there, it can throw your entire endocrine system into chaos.
The most common type of these tumors is the prolactinoma. It’s not cancer, but it’s powerful. Prolactinomas make too much of the hormone prolactin - the same hormone that tells your body to make breast milk after childbirth. When this happens outside of pregnancy, things go sideways fast.
What Happens When Prolactin Gets Too High?
High prolactin doesn’t just cause one symptom. It rips through multiple systems in your body. In women, it often stops periods entirely. Some notice milk leaking from their breasts even if they’ve never had a baby. Others struggle with infertility, low libido, or bone thinning because estrogen drops. In men, the signs are quieter but just as serious: erectile dysfunction, reduced body hair, lower muscle mass, and sometimes breast enlargement. About 80% of men with prolactinomas report sexual problems. And here’s the thing - many people don’t realize these are signs of a tumor. They think it’s stress, aging, or bad luck.
Why does this happen? Prolactin suppresses the hormones that drive ovulation and testosterone production. When levels climb above 150 ng/mL, the chance that it’s a prolactinoma jumps to 95%. Levels over 200 ng/mL almost always mean the tumor is larger than 1 cm - a macroadenoma. These bigger tumors can press on nearby nerves, especially the optic chiasm. That’s when vision problems start: blurry side vision, tunnel vision, or even partial blindness if left untreated.
How Do You Know You Have One?
Diagnosis starts with a blood test. Not just any prolactin test - you need to avoid stress, nipple stimulation, or even a recent breast exam before the draw. A single high reading isn’t enough. Doctors repeat it, check thyroid function (because hypothyroidism can mimic this), and rule out medications like antidepressants or antipsychotics that raise prolactin.
If levels stay high, an MRI of the pituitary is next. It’s not a regular brain scan. You need a special 3mm slice MRI with contrast to catch even tiny tumors. A microadenoma is under 1 cm. A macroadenoma is over 1 cm. About 80% of these tumors are small. But even small ones can cause big problems.
For tumors bigger than 1 cm, an eye exam is mandatory. Visual field testing checks for blind spots. If you’re losing side vision, time matters. Delaying treatment can lead to permanent damage.
First-Line Treatment: Pills That Work
For prolactinomas, the first move isn’t surgery. It’s medicine. Specifically, dopamine agonists. These drugs trick your brain into thinking there’s enough prolactin already. The two main ones are cabergoline and bromocriptine.
Cabergoline is the gold standard. It’s taken twice a week - 0.25 mg to start. Most people see prolactin levels drop within weeks. By three months, 80-90% of microadenomas are back to normal. Tumors shrink by 70% or more in most cases. One patient from Mayo Clinic had a 2.4 cm tumor with prolactin at 5,200 ng/mL. After six months on cabergoline, her levels fell to 18 ng/mL. That’s not a fluke. It’s routine.
Bromocriptine works too, but it’s harder to tolerate. Up to 40% of users quit because of nausea, dizziness, or low blood pressure. Cabergoline? Only 18% stop due to side effects. That’s why guidelines from the Endocrine Society say cabergoline should be first for everyone.
But here’s the catch: most people need to stay on it for years. About 70% of patients can’t stop without prolactin rebounding. Some take it for life. That’s okay - as long as you’re monitored.
When Surgery Comes Into Play
Surgery isn’t the first choice - but it’s critical for some. If your vision is failing, or if you can’t take the pills, or if the tumor doesn’t shrink after six months of medication, then surgery is next.
The procedure is called transsphenoidal. It’s done through the nose. No scalp incisions. No visible scars. Endoscopic tools let surgeons see the tumor clearly. For microadenomas, success rates hit 85-90%. For macroadenomas? It drops to 50-60%. Why? Because big tumors often grow into the cavernous sinus, wrapping around nerves and blood vessels. You can’t always remove them all.
Recovery is fast - usually 3 to 5 days in the hospital. But risks are real. Cerebrospinal fluid leaks happen in 2-5% of cases. Diabetes insipidus (a temporary condition where you pee too much) affects 5-10%. And in rare cases, the tumor bleeds suddenly - pituitary apoplexy. That’s an emergency.
Even after successful surgery, prolactin can creep back. Recurrence rates are 5% for small tumors but jump to 25-30% for large ones. That’s why follow-up blood tests every 3-6 months are non-negotiable.
Radiation: A Last Resort
Radiation isn’t used much anymore - but it’s still there for stubborn cases. It’s slow. It takes 2 to 5 years to work. And it’s not gentle. About 30-50% of people end up with low hormone levels afterward - meaning they’ll need lifelong replacement therapy for cortisol, thyroid, or sex hormones.
There are two types: conventional radiation and Gamma Knife. Conventional radiation spreads beams over weeks. Gamma Knife delivers one high-dose shot with pinpoint accuracy. It’s better for small tumors near the optic nerve. Tumor control is 95% at five years. And damage to the optic nerve? Only 1-2% with Gamma Knife versus 5-10% with older methods.
But here’s the reality: most patients don’t choose radiation unless everything else failed. It’s not a quick fix. It’s a long game.
What About Long-Term Risks?
Cabergoline is safe for most. But if you take more than 2 mg per week for over three years, your heart valves can thicken. The European Society of Endocrinology recommends an echocardiogram every two years for those on high doses. It’s rare - 2-7% risk - but real.
And here’s something few talk about: the emotional toll. People with prolactinomas often feel invisible. Women with no periods or milk leakage feel embarrassed. Men with low libido feel emasculated. Many avoid intimacy. Depression and anxiety are common. Support groups matter. One Reddit community of over 1,200 patients found that 78% felt better within six weeks of starting cabergoline. That’s hope.
What’s Next?
New drugs are coming. Paltusotine, a new oral pill, is in trials for prolactinomas. It might replace cabergoline in the next five years. Researchers are also exploring gene therapy - targeting mutations like GNAS and USP8 that make tumors grow. AI is helping surgeons plan better paths through the skull. And in five years, doctors may test your tumor’s DNA before choosing treatment - not just guess based on size.
But for now, the rules are simple: test prolactin early. Don’t ignore missed periods or low sex drive. Start with cabergoline. Monitor closely. Don’t stop pills without talking to your doctor. Missing a dose can spike prolactin in 72 hours. And always, always get that MRI if symptoms persist.
Can prolactinomas cause infertility?
Yes. High prolactin blocks ovulation in women and lowers testosterone in men, which reduces sperm production. In women, about 95% of prolactinomas cause amenorrhea (no periods). In men, 80% experience sexual dysfunction. But the good news? Most regain fertility within months of starting dopamine agonists like cabergoline.
Is a prolactinoma cancer?
No. Prolactinomas are benign tumors. They don’t spread to other organs like cancer. But they can grow large enough to press on the brain, optic nerves, or surrounding structures. That’s why they need treatment - not because they’re malignant, but because they disrupt hormone balance and can damage vision or fertility.
Why does cabergoline work better than bromocriptine?
Cabergoline lasts longer in the body, so it’s taken just twice a week. Bromocriptine needs daily dosing and causes more nausea, dizziness, and low blood pressure. Studies show cabergoline normalizes prolactin in 80-90% of cases versus 70-80% for bromocriptine. It also shrinks tumors more effectively and has fewer side effects - making it the preferred first-line treatment.
Can you stop taking cabergoline after your prolactin normalizes?
Sometimes, but rarely. About 70% of patients relapse if they stop. Doctors may try to taper the dose after 2-3 years of normal levels and stable MRI results, but most patients need to stay on it long-term. Stopping suddenly can cause prolactin to spike within 72 hours, bringing back symptoms.
How often should you get your prolactin checked?
When starting treatment, check every month until levels stabilize. After that, every 3-6 months for the first year. If everything stays normal for two years, annual testing is usually enough. MRI scans are repeated every 6-12 months initially, then every 2-3 years if the tumor is shrinking and prolactin is stable.
Are there natural ways to lower prolactin?
No. While stress reduction and avoiding nipple stimulation can help prevent temporary spikes, they won’t shrink a tumor or fix a true prolactinoma. Only dopamine agonists like cabergoline reliably lower prolactin and shrink the tumor. Don’t rely on herbs, supplements, or diets - they don’t work for this condition.
What You Should Do Next
If you’re experiencing unexplained missed periods, breast milk without pregnancy, low libido, or vision changes - get tested. Don’t wait. A simple blood test can change everything. If prolactin is high, insist on an MRI. If it’s confirmed, start cabergoline. Stick with it. Monitor. And remember: this isn’t a life sentence. It’s a manageable condition. Thousands recover fully. You can too.
Andrew Poulin
March 6, 2026 AT 23:42One dose changed everything for me.
Weston Potgieter
March 7, 2026 AT 03:08Vikas Verma
March 7, 2026 AT 21:04Sean Callahan
March 8, 2026 AT 01:40anyone else feel like a lab rat?
Ferdinand Aton
March 9, 2026 AT 10:33Tim Hnatko
March 9, 2026 AT 22:34William Minks
March 11, 2026 AT 19:32Jeff Mirisola
March 12, 2026 AT 21:29Susan Purney Mark
March 12, 2026 AT 21:47Ian Kiplagat
March 14, 2026 AT 21:27Amina Aminkhuslen
March 16, 2026 AT 19:38amber carrillo
March 17, 2026 AT 03:47Aaron Pace
March 17, 2026 AT 07:45